
 Play2Box
Play2Box












Cervical Spine Anatomy - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the Anatomy of the Cervical Spine.
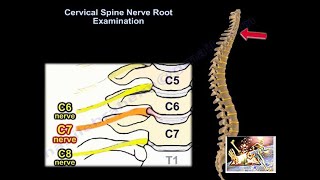
C1 is a ring. At the upper cervical region, the spinal canal is 2.5 times larger than the cord size. 50% flexion-extension is between occiput & C1. 50% of neck rotation is between C1 and C2. C5-C6 is more prone to disc degeneration due to anatomical and mechanical forces centered at this level. There are 8 cervical nerve roots. These nerves exit on or above each vertebra C8 exits above T1. Disc prolapse occurs due to rupture of the annulus fibrosus and protrusion of the nucleus pulposus which compresses the nerve root. The most common type of disc prolapse is posterolateral disc prolapse. C2 ganglion may be vulnerable to compression/entrapments due to:
•Cervical arthritis causing repeated mechanical damage or compression
•Post traumatic hyperextension injuries (whiplash injury)
•C2 Ganglion entrapment/ compression causes cervicogenic headache
The incidence of vertebral artery increases if the fracture extends into the foramen transversum. This may manifest as impaired consciousness, drowsiness, syncope, ataxia, brain-stem and cerebellar ischemia/infarction, dysarthia, headache, vertigo, visual impairment, and ptosis. Bilateral or dominant vertebral artery injury can cause fatal ischemic damage to the brain stem and cerebellum. Delayed cortical blindness and recurrent quadriparesis can also occur from occult vertebral artery injury after cervical trauma. The great majority of vertebral artery injuries are clinically silent. The majority of patients with vertebral artery injuries had flexion-distraction or flexion-compression types of spinal injuries.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
